
Bax’s Private War
Editor’s Note: The Bax Website is proud to offer the following article to commemorate the 70th anniversary this month (October 2023) of Sir Arnold Bax’s death by Dr. Claire Colebourn FRCP. This article is based on a scientific article being published in the Journal of the American College of Cardiology. Dr. Colebourn is a Consultant Critical Care Physician at University Hospitals Oxford and the current President of the British Society of Echocardiography.
Bax’s Private War
When a story is retold enough times, there comes a point when you stop asking yourself, but is it true?
This was one of the deepest lessons I learnt when I was training in medicine. I was told a story about a man who had such thick medical notes they had to be brought into clinic on their own trolley. According to the hallowed wisdom contained within, this poor man had a particularly nasty and terminal diagnosis.
Except he didn’t… each letter written about him and each conversation with him began with the ‘known’ diagnosis, at some point everyone stopped questioning the label that he had been given and accepted it as the truth. Received wisdom is hard to shift.
Sir Arnold Bax KVCO, Master of the Kings Musick, triple doctorate holder, writer, poet and musical ‘man for all seasons’ is surrounded by a rhetoric which fascinates me as a physician. Bax has been type-cast into the image of a hedonistic heavy drinker. He is written into history as aloof to the society and establishment he appeared to desire respect from.
But the medical truth of Bax’s life runs absolutely counter to this characterisation.
This story really begins with Bax’s tone-poem ‘November Woods’; Bax’s formidable musical description of anguish and love inspired while he waited for Harriet Cohen near Amersham station in November 1916. Fascinated to find out where November Woods actually are, I started my search with his biographies and like every ‘dedicated’ reader I flicked straight to the pictures in the centre of the book…
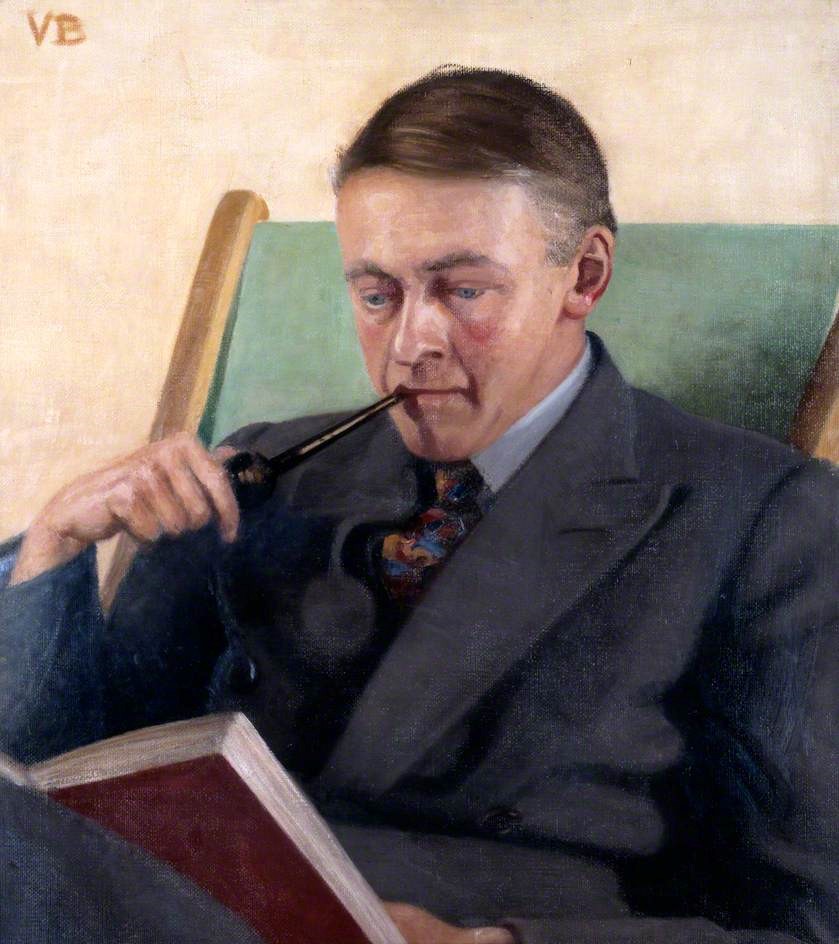
Bax was anelfin and handsome young man whose appearance morphed dramatically into a heavily jowled 50 year-old with weight curiously distributed towards his legs. These are not normal ageing changes for a man. But his facial changes are even more interesting; his cheeks later marked with two lurid patches clear even in black and white photographs. My interest now seriously piqued I wanted to see a colour picture. A quick internet trawl provided a diamond amongst the rhinestones of airbrushed record covers – a colour portrait in oil. This is such an important artefact from Bax’s life, not because of the sitter, but because of the artist.
Medical practice is essentially based on one single over-riding principle; to diagnose accurately we must directly observe and examine the patient, and that is how I ended up balanced precariously on a piano stool in the Arnold Bax room at the Royal Academy of Music looking directly into the eyes of my ‘patient’.
Vera Bax knew her brother-in-law so well that she painted him exactly as she knew him with fuschia cheeks and ears but a small strip of normal skin between the nose and cheeks. Looking at Vera’s brushwork I was impressed by her scientific accuracy; the medical term for this appearance is a ‘malar flush’ and it signifies the potential of an underlying cardiac condition causing ‘pulmonary hypertension’ (high pressure in the right side of the heart and the vessels supplying blood to the lungs). Pulmonary hypertension has many causes and guises, but it often causes life-changing symptoms. If this is what Bax was suffering from then the next questions are, how bad were his symptoms and what was the cause?
Truly diagnostic facts from Bax’s unusual childhood are scant but we can start to build up a picture. The first-born son of wealthy parents he was educated at home with his brother in the care of his tutor until he joined the RAM in 1900. During Bax’s childhood, teens and twenties accounts of his life paint a picture of an essentially normal exercise capacity. Isolated incidents of collapsing at the wicket on a hot day, seeing a doctor twice during his teens, on both occasions with little concrete documentation, and describing his own awareness of his heart beating wildy during his first serious romantic encounter do not add up to diagnostic fact.
But the second big clue comes in a comment made by Bax’s brother Clifford in his biographical note when he uses the phrase ‘usual palpitations’. (Palpitations describe the exaggerated sensation of your own heart-beat.) “Usual” is such an interesting word for Clifford to choose.
So far, we have two significant factors suggesting that Bax has long-standing heart disease but we need much more to make a diagnosis and understand its impact on him. But then, the dark menace of the First World War sweeps into Europe and blows the dust from Bax’s story.
In July 1915 Bax was examined by a Dr Lewis G Glover of Belsize Park Hampstead apparently to determine his suitability for military service. Glover declared Bax unfit for military service due to his ‘nervous temperament’. If we read Glover’s assessment in isolation it leaves us wondering if this declaration was the sole intention of the consultation, affecting our view of Bax’s character. However, from a medical perspective this information is mediocre at best.
But in 1916, mediocrity is replaced by gold-dust and into Bax’s life strides our second knight, the pre-eminent cardiologist and physician of his day, Sir James Mackenzie FRSM.
Mackenzie is to medicine what Mozart is to music, and he deserves a fitting fanfare.
Mackenzie was a meticulous observer and raised the standard of medical practice to forensic levels. When I pick up my stethoscope today, I still use Mackenzie’s processes exactly as he did. The Mackenzie medal remains the highest honour in British cardiology, awarded to the elite of the profession. In a Victorian world without telecommunication Mackenzie’s reputation and reach was staggering; the American College of Cardiology being created in his honour. Mackenzie had deep experience of structural heart disease and he published the original descriptions of the heart rhythm disturbances that caused Bax’s palpitations; Bax could not have picked a more exacting medical opinion.
At the time he met Bax, Mackenzie had been engaged by the War Office to investigate the condition known as ‘soldiers’ heart’ in men returning from the front. Mackenzie published a memorandum to guide doctors examining recruits in the British Medical Journal. The focus of Mackenzie’s work was to remobilise men, not demobilise them. He disagreed with the concept that the presence of a heart murmur should preclude a man from active service. If Mackenzie thought Bax physically capable of military service he would have sent him to war.
Our two knights met each other only once on the 14th of September 1916 in Mackenzie’s rooms at 133 Harley Street, London.
Mackenzie’s examination findings were typed up and then signed in ink to verify their origin: ‘J Mackenzie FRSM’. The report is later stamped with two official stamps of the National Review Board dated 29th Jan 1917 and then 22nd of June 1918, indicating that the report was brought by Bax to annual medical review boards in the years that followed. No physician of the day would have considered over-ruling Mackenzie; you don’t tell Mozart he’s got his bar-lines in the wrong place.
Mackenzie’s report reads verbatim as follows;
‘I certify that I have examined Mr Arnold Bax. He is manifestly a very nervous man, and suffers much from palpitation and breathlessness on very slight exertion. During the examination his pulse was very excitable, and at times very irregular, the irregularity being due to frequent occurrence of extra-systoles. The apex beat was large and diffuse, and extended one inch beyond the nipple line; there was a rough systolic murmur best heard at the base. He also suffers from a curious mental condition in which there is fear of being in enclosed spaces (claustrophobia). These symptoms point to a condition of ill health that renders him in my opinion totally unfit for military service.’ J Mackenzie MD FRSM.
When I read this report for the first time in the British Library, I felt the oppressive gravity of what I was reading. Mackenzie’s report, typed on thick pale blue cartridge paper looks like it has been folded and unfolded many times, being read and re-read by its owner and presented to a progression of Review Board physicians.
After Bax’s death Harriet spent many months curating important documents from his life. She appears to have recognised the pivotal importance of this document preserving it next to his Knighthood and the certificate of his office as the Master of the Kings Musick.
Harriet would have noticed the overt symptoms described so precisely by Mackenzie. The years of the First World War were arguably the most intense years of their relationship. Bax regularly cycled to Amersham from Beaconsfield and then walked up Amersham hill through November Woods to meet her. This would have been increasingly challenging for him and Harriet would have noticed this. There is no written record of Bax and Harriet discussing the outcome of his consultation with Mackenzie. Harriet’s letters tell us that at the time of the consultation she was staying with Bax’s cousin Freda, raising the possibility that Bax sent her there to maintain his privacy around his consultation with Mackenzie. It is therefore possible that Bax never shared Mackenzie’s findings with Harriet in life, the focus of his letters being on her health and not his.
Mackenzie’s findings are diagnostic of a ‘hole in the heart’ between the two main pumping chambers which are called the right and left ventricles: the medical term for this is a ‘ventricular-septal defect’. The murmur is caused by turbulent blood flowing through the hole. This is one of the commonest congenital heart conditions we see and in the modern era they are usually picked up at routine screening and monitored or corrected as required; small holes often require no intervention at all. In the pre-surgical era (pre-1970s) this was not a luxury available to Bax.
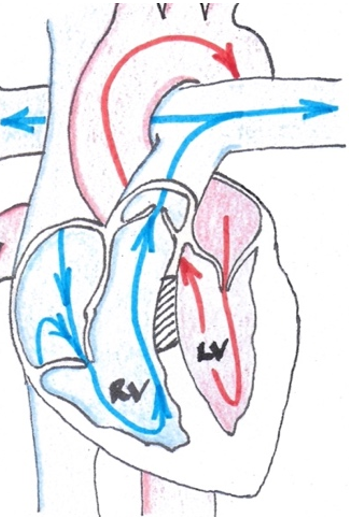
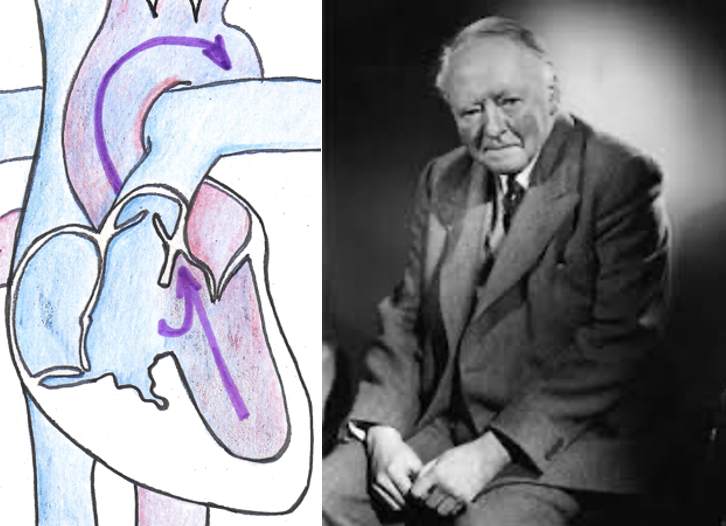
The diagram below helps you visualise blood flow through the normal heart. Low oxygen containing blood (blue arrows in this diagram) flows under low pressure into the right atrium and then into the right ventricle (RV below). Blood flows out of the right ventricle into the pulmonary arteries which take blood to the lungs to be re-stocked with oxygen. The red arrows show the flow of re-oxygenated blood being pumped into the great arteries and around the body by the powerful left ventricle (LV below). The hatched area shows the location of a ventricular-septal defect; a hole in the wall between the ventricles.
To give you a quick tour of the work of the ventricles; the right one is essentially the servant of the left. The right ventricle carefully monitors and delivers the exact volume of blood that the main heart pump – the left ventricle – needs to do its job. Imagine the left ventricle as the ‘shire horse’ of the heart; strong, relentless and capable of delivering extraordinary levels of muscular work on demand. This will help you understand Mackenzies’ findings.
The effect of a hole in the heart depends upon its size. Very small ones are common and often cause no problems at all. We can fairly accurately estimate the size of the hole in Bax’s heart to be 18-20mm by looking at his life-span and his symptoms: Bax’s physical and compositional capacity mirrored his heart in three main phases:
Phase I: Compensated phase (1903-1920)
In the early part of this phase Bax’s symptoms are mainly palpitations caused by high pressure blood going through the hole and hitting the right heart wall (this is the word ‘extra-systoles’ which Mackenzie uses). The direction of blood flow through the hole is simply determined by the pressure gradient. At this point blood flows through the hole from the high pressure left ventricle into the low pressure right ventricle.
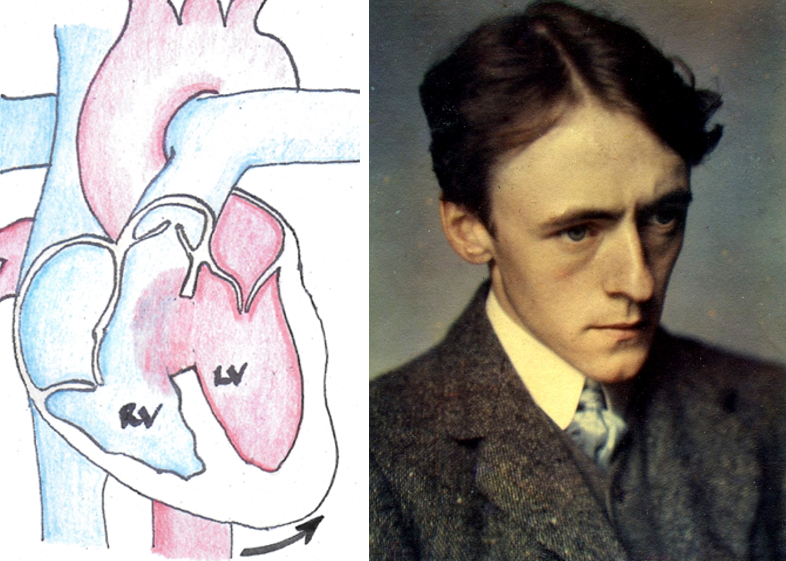
Palpitations would have made Bax feel distracted and uncomfortable, and this would have been worse in stressful situations. His exercise capacity however, would have been fairly normal since the strong left ventricle compensates for the abnormal flow through the hole by expanding in the direction shown by the arrow. This compensatory mechanism maintains the proportion of blood flowing through the normal exit channel and round the body. Bax’s appearance at this time is of a young fit man as seen in the photograph below. (Bax photographed by Paul Corder.)
When Bax was examined by Mackenzie towards the end of this period in 1916, he was much more symptomatic, becoming breathless with minimal effort. Mackenzie found the ‘apex beat’ (which marks the position of the left ventricle in the chest) to be very displaced from its normal position; it has reached maximal compensation. Mackenzie noted the frequency of Bax’s palpitations and diagnosed their cause (extra-systoles = irregular extra heart beats).
From a compositional perspective during this period of his life Bax wrote over 1000 hours of music with a fairly even mix between orchestral works, chamber and instrumental music, songs and piano solos.
Phase II: Pulmonary hypertension phase (1920-1939)
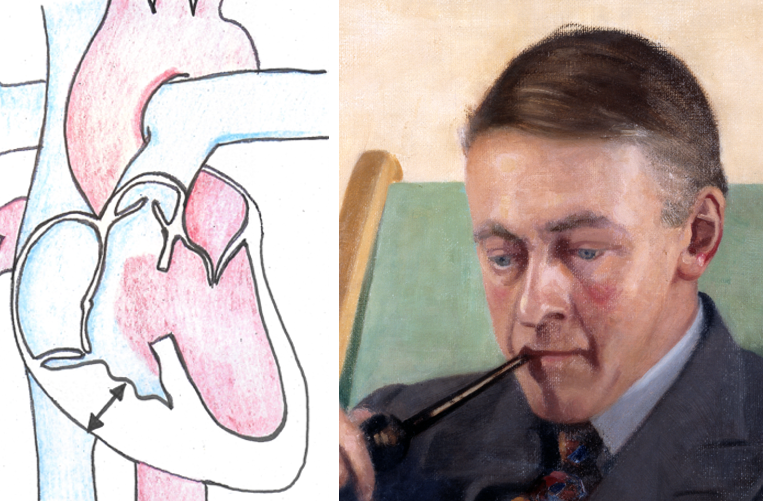
The cracks are really beginning to show. The size of the hole in Bax’s heart means that the right ventricle has started to change in structure. It is thickening its wall to cope with the constant bombardment of blood coming through the hole, as shown by the arrows in the diagram, and the pressure is gradually rising on the right side of the heart. This rise in pressure is being transmitted through the blood vessels which deliver blood to the lungs. High pressure on the right side of the heart is known as pulmonary hypertension and this is very likely the cause of the malar flush which Vera painted on Bax’s portrait (shown below). (Reproduced with permission from the RAM.)
During this phase Bax would still have suffered from palpitations which would have been progressive. In addition to this he would have become breathless on even minimal physical effort. The progressive pressure rise in his right heart would have caused congestion of the veins in his legs and liver, changing his body shape. Bax describes this situation precisely in the foreward to his autobiography; one of few moments when he lets his guard down and talks about his own health;
‘The tragi-comedy of the body! ‘I resent the buzzing of blood in my temples whenever I stoop to tie a shoelace or pick up my pen from the floor: the thickening of tissue beneath the skin in front of my ears and under my chin; the degrading fact that in order to rise from my deep arm-chair I needs must huddle my trunk forward and lever myself up by pressing hard upon the arms.’
Compositionally, this period marks Bax’s most prolific phase and this may be in part related to his need to find sedentary occupation. From 1920-1939 Bax wrote over 2000 minutes of music including his seven symphonies. The focus of his work during these years was orchestral and chamber or instrumental music.
Phase III: Severe pulmonary hypertension phase leading to shunt reversal 1939-1953
After 1939 there is a precipitous drop in Bax’s compositional output: he wrote only 320 minutes of music in his final 14 years of his life despite being at the peak of his powers as a composer. This likely coincides with the onset of the final phase of Bax’s illness as his pulmonary hypertension progressed.
At some stage in this period of his life, the muscular overgrowth of the right ventricle, and the pressure on the right side of the heart would have become so severe that it began pushing blood the wrong way through the hole. This means that low oxygen blood was being pumped around the whole body by the left ventricle: the blood is essentially bypassing the lungs. The medical term for this is ‘shunt reversal’ or Eisenmenger’s syndrome. This is shown in the diagram below.
During this period Bax would have felt light-headed, exhausted and very unwell. Progressive severe pulmonary hypertension and then shunt reversal would have blunted his intellect and made even light physical work a huge effort. This is reflected in Bax’s physical appearance from this time shown in the photograph above. Bax’s shuffling walk and ruddy complexion are described by Mrs Elinson Hedwig Stein who lived in Storrington at the same time as Bax and was shocked by the change in his appearance having known him as a fitter young man.
Over time as Bax’s blood oxygen levels gradually fell he would have become slate grey and then blue as his shunt reversal worsened. Initially this would appear only with physical effort and then at rest towards the very end of his life. Tilly Fleischmann provides us with a poignant first-hand account describing her shock on seeing Bax one day after his death looking healthier than he had in years! This is typical of the appearance of people with low oxygen saturations; when the grey-blue colour disappears, through whatever means, they look better.
It is important to note that in both phase II and III Bax would have been physiologically intolerant of more than a small amount of alcohol. Alcohol is a ‘systemic vasodilator’, this means it opens up blood flow throughout the body making the circulation work even harder and exacerbating the volume of blood being shunted, dramatically worsening his symptoms.
It is a very common misconception that the ruddy cheeks of pulmonary hypertension are due to excessive alcohol. This is often how people are mislabelled even today. Coupled with a shuffling gait and intermittent confusion due to low oxygen levels you can see how the wrong conclusion could easily be reached. Bax’s circulation was balanced on a knife-edge and he would have become expert at staying within tight lifestyle tram-lines to stabilise his symptoms.
But examining the patient and making a diagnosis is only part of what a physician does. Mackenzie would have carefully explained Bax’s diagnosis to him including what lay ahead. Mackenzie’s nickname was ‘beloved physician’, a testament to his kindness with his patients. Mackenzie waived his examination fee that day; he had given Bax life-changing and very distressing news. Bax never met Mackenzie again. The die was cast.
Bax knew death was a daily threat as the years wore on. His letters describe waking in the early hours of the morning and feeling desperately ill. This is a symptom of having low oxygen levels which naturally drop further at night. He describes feeling the ‘snub-nose of death’ approaching him in one very distressed letter written in 1948. Despite his inner distress Bax was perpetually supportive to those he loved finding clever ways of keeping his incapacity covered up as much as he could. You have to love him for that; a private hell faced with a wistful smile.
When death came Bax clearly knew that he had reached the final turn, giving the Fleischmann children his beloved Turkish Delight to share amongst themselves. On his last day he was driven by John Horgan at his request to take one last look at the sunset at Kinsale Head. Declaring that he felt extremely unwell, Bax was driven back to the Fleischmann’s house where he was staying.
John Horgan wrote a first-hand account of Bax’s death just five days afterwards providing us with a high-quality eye-witness statement. The account paints a picture of the process of death from end-stage pulmonary hypertension describing Bax as ‘blue and breathing heavily’. Mrs Fleischmann, herself a qualified doctor, recognised how unwell Bax was and summoned the local senior physician Professor James O’Donovan, who was powerless to alter the inexorable trajectory of Bax’s uncorrected ventricular-septal defect. Bax died quietly at 9.30pm muttering his thanks to the doctor.
In the absence of a post-mortem Bax’s death certificate reads ‘cardiac infarction’ which does not reflect Mackenzie’s findings or Bax’s physical symptoms or mode of death. Eisenmenger’s syndrome really only entered medical practice through the cardiologist Paul Wood in 1951 making it very unlikely that the attending physician Professor James O’Donovan would have seen another case or recognised it in Bax.
To fully understand the arc of Bax’s life and legacy you have to deeply understand the man. You have to walk in his shoes. Bax did not live alongside his illness, he cohabited with it every day. He never gave a speech or conducted any of his own symphonies simply because he couldn’t.
Bax’s true biography, written by his own compositional output and painstakingly catalogued by Graham Parlett, graphically reflects not only the three phases of an uncorrected ventricular-septal defect but also the actions of a man who was told in 1916 that time was limited. From that point onwards we see him laying down the legacy of his seven great symphonies, a phenomenal output in 21 years. Bax knew he was in a race against time.
Visibility is power, but such physical self-promotion was not an option for Bax. From 1920 onwards as each day passed his functional capacity and presence in musical society lessened. From the age of 56 his huge intellectual level and his ability to cement his legacy fell away from him with his dropping oxygen levels.
Written so soon after his consultation with Mackenzie I now listen to ‘November Woods’ with a new understanding of the pain he was feeling. Bax wrote to Earnest Newman prior to the first performance of the work;
‘If there are sounds in the music which recall the screaming of the wind and cracking of strained branches, I hope they may suggest deeper things at the same time. The middle part may be taken a dream of happier days, such as sometimes come in the intervals of stress either physical or mental.’
Despite the many other valid and well documented factors affecting the reach of Bax’s work we must consider the physical, psychological and intellectual impacts of his life-long battle and the news that Mackenzie gave him that day, as central to the man he was capable of being.
Sir Arnold, thank you for the legacy you gave us.
Dr CL Colebourn FRCP
September 2023
This narrative is based on the case report ‘Bax and Mackenzie, two knights, one war and a lost legacy’ which can be accessed with full references through the Journal of the American College of Cardiology (currently in press).